For decades the random 12-core biopsy has been the standard of care for diagnosing prostate cancer. What most men don’t know is that random biopsy can be dangerous and its results can be misleading. Fortunately, there are now better ways to interpret a high PSA that are less invasive, safer, and more accurate.
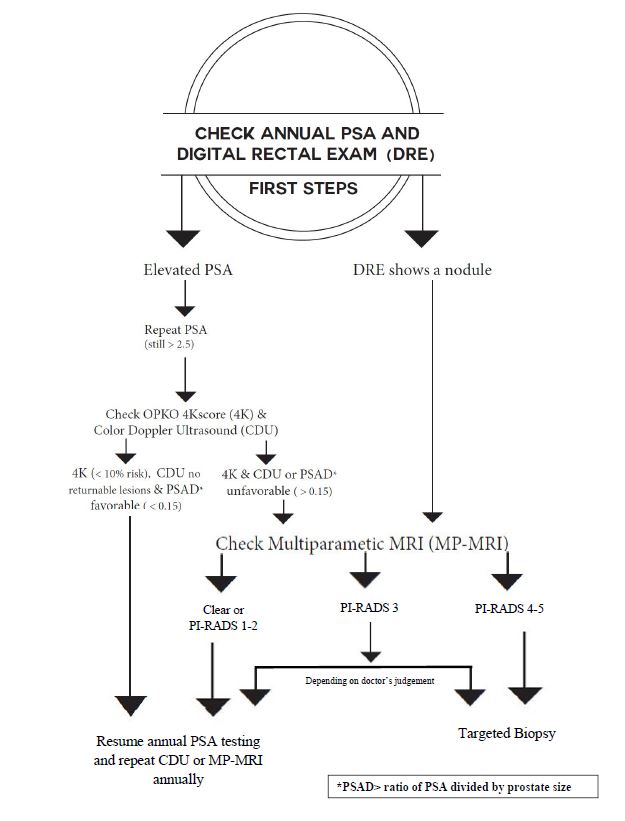
The following flowchart shows the proper steps to take when faced with an elevated PSA.
PSA (prostate-specific antigen)
PSA is a blood test that is used to screen for prostate cancer. PSA can be elevated from other causes such as BPH, prostatitis, recent sexual activity, lab error, Low-Grade prostate cancer (Gleason 6), or consequential prostate cancer (Gleason 7+). After treatment, PSA is used to monitor treatment success. Explore PSA.
DRE (digital rectal exam)
The DRE, also called the finger exam, helps doctors determine if there are any irregularities in the gland, such as an abnormally shaped gland, enlargement, or nodules. The results of the DRE are called the clinical stage, or the T stage.
OPKO 4Kscore
OPKO 4Kscore is a blood test that predicts when a high PSA is caused by clinically significant prostate cancer. Other prostate cancer biomarker tests available are Select MDx and ExoDx.
PSAD (PSA density)
Benign enlargement of the prostate gland is common as men age. As a general rule, the bigger the prostate, the more PSA it produces. To determine if an elevated PSA is higher than expected for an enlarged prostate, there is a simple rule of thumb to follow: the prostate size should be in a ten-to-one ratio with the PSA. For example, a normal PSA for a 40 cc prostate is about 4. For a 70 cc prostate, a PSA of 7 can be considered normal.
PSA density is considered abnormal when it is 50% higher than expected. If you do the inverse equation, and divide the gland volume by the PSA, an abnormal PSA will be anything above 0.15.
CDU (Color Doppler Ultrasound)
Color Doppler ultrasounds can help doctors determine the size of the prostate and may indicate if there are any suspicious lesions in the gland that may be indicative of a prostate cancer.
MP-MRI (3T multiparametric MRI)
3T MP-MRI is an imaging scan that uses contrast to locate suspicious lesions in the prostate. It can show if the cancer is spreading beyond the prostate capsule, or has spread to the seminal vesicles. An MRI is only a valid substitute for a biopsy when performed at a validated expert facility.
PI-RADS (Prostate Imaging Reporting and Data System)
Imaging results are reported as PI-RADS category 1-5, indicating the likelihood that the suspicious area contains a clinically significant prostate cancer (Gleason 7+).
- PI-RADS 1: Very low
- PI-RADS 2: Low
- PI-RADS 3: Intermediate (undetermined)
- PI-RADS 4: High
- PI-RADS 5: Very High
TARGETED BIOPSY/IMAGE-GUIDED BIOPSY
A targeted biopsy takes only two-to-three cores, and is directed at the lesion of concern based on the findings of the MP-MRI or color Doppler ultrasound. Because of the fewer cores, a targeted biopsy tends to be a safer, more accurate option.
Isn’t the new ExactVu 29mhz ultrasound much better than CDU?
ExactVu is a gray scale ultrasound only, this means that it does not look at tumor vascularity. The benefit of color Doppler is that it uses both grey scale and Doppler (which examines tumor vascularity). Also, the skill of the doctor who is administering and interpreting the ultrasound images needs to be high quality as well.